Twin Pregnancy Complete Guide 2025 Causes Types Diagnosis Risks and Management
Below is a **complete, detailed, SEO-friendly medical article on Twin Pregnancy**, written **without images**, structured with clear **H1–H3 headings**, and optimized for **search engines and medical learning**.
---
## **SEO Title**
Twin Pregnancy Complete Guide 2025 Causes Types Diagnosis Risks and Management
---
## **Meta Description**
Comprehensive medical guide on twin pregnancy covering types, causes, diagnosis, antenatal care, complications, fetal surveillance, delivery planning, and prognosis for mother and babies.
---
## **SEO Keywords**
twin pregnancy, multiple pregnancy twins, dichorionic twins, monochorionic twins, twin pregnancy diagnosis, twin pregnancy complications, twin pregnancy antenatal care, twin pregnancy delivery, twin pregnancy risks, twin pregnancy management, twin gestation obstetrics
---
# **Twin Pregnancy**
## **1. Definition**
Twin pregnancy is a type of **multiple gestation** in which **two fetuses develop simultaneously in the uterus**. It carries **higher maternal and fetal risks** compared to singleton pregnancy and requires **specialized antenatal monitoring and delivery planning**.
---
## **2. Epidemiology**
* Incidence: **1 in 80–90 pregnancies**
* Higher incidence with:
* Assisted reproductive techniques
* Advanced maternal age
* Family history of twins
* Multiparity
---
## **3. Classification of Twin Pregnancy**
### **3.1 Based on Zygosity**
* **Dizygotic (Fraternal) Twins**
* Fertilization of two separate ova
* Always dichorionic and diamniotic
* Most common type
* **Monozygotic (Identical) Twins**
* Division of a single fertilized ovum
* Chorionicity depends on timing of division
---
### **3.2 Based on Chorionicity and Amnionicity**
#### **3.2.1 Dichorionic Diamniotic Twins (DCDA)**
* Two placentas, two amniotic sacs
* Lowest complication rate
* May have fused placentas
#### **3.2.2 Monochorionic Diamniotic Twins (MCDA)**
* One placenta, two amniotic sacs
* Risk of twin-to-twin transfusion syndrome
#### **3.2.3 Monochorionic Monoamniotic Twins (MCMA)**
* One placenta, one amniotic sac
* Highest risk
* Cord entanglement common
---
## **4. Etiology and Risk Factors**
* Assisted reproductive technology
* Ovulation induction
* Maternal age above 30 years
* African ethnicity
* Tall stature and high BMI
* Family history of twins
---
## **5. Diagnosis of Twin Pregnancy**
### **5.1 Clinical Features**
* Excessive uterine enlargement
* Severe nausea and vomiting
* Early perception of fetal movements
* Palpation of multiple fetal parts
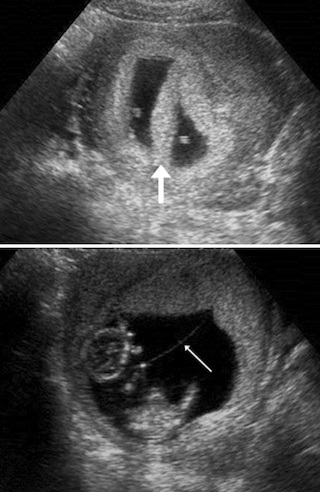
### **5.2 Ultrasonography**
* Gold standard for diagnosis
* Confirms:
* Number of fetuses
* Chorionicity and amnionicity
* Gestational age
* Placental location
### **5.3 Doppler Studies**
* Used for fetal surveillance
* Essential in monochorionic twins
---
## **6. Antenatal Care in Twin Pregnancy**
### **6.1 General Principles**
* More frequent antenatal visits
* Early booking
* Multidisciplinary approach
### **6.2 Nutritional Requirements**
* Increased calorie intake
* Iron supplementation
* Folic acid
* Calcium and protein supplementation
### **6.3 Fetal Surveillance**
* Serial growth scans every 2–4 weeks
* Amniotic fluid assessment
* Doppler velocimetry
---
## **7. Maternal Complications**
* Anemia
* Gestational hypertension
* Preeclampsia
* Gestational diabetes
* Antepartum hemorrhage
* Polyhydramnios
* Increased operative delivery
* Postpartum hemorrhage
---
## **8. Fetal Complications**
* Preterm birth
* Low birth weight
* Intrauterine growth restriction
* Congenital anomalies
* Twin-to-twin transfusion syndrome
* Cord accidents
* Perinatal mortality
---
## **9. Special Complications in Monochorionic Twins**
### **9.1 Twin-to-Twin Transfusion Syndrome**
* Unequal placental blood flow
* Donor twin: growth restriction, oligohydramnios
* Recipient twin: polyhydramnios, cardiac overload
### **9.2 Twin Anemia Polycythemia Sequence**
* Chronic intertwin blood transfusion
* Diagnosed by Doppler MCA PSV
---
## **10. Management of Twin Pregnancy**
### **10.1 Antenatal Management**
* Strict blood pressure monitoring
* Early detection of complications
* Corticosteroids for lung maturity if preterm risk
### **10.2 Timing of Delivery**
* DCDA twins: 37–38 weeks
* MCDA twins: 36–37 weeks
* MCMA twins: 32–34 weeks by planned cesarean
### **10.3 Mode of Delivery**
* Vaginal delivery if:
* First twin cephalic
* No obstetric contraindications
* Cesarean section if:
* First twin non-cephalic
* Monoamniotic twins
* Obstetric complications
---
## **11. Intrapartum Care**
* Continuous fetal monitoring
* Availability of neonatal intensive care
* Skilled obstetric and anesthetic support
---
## **12. Postpartum Care**
* Active management of third stage
* Monitoring for postpartum hemorrhage
* Lactation support
* Neonatal care for prematurity
---
## **13. Prognosis**
* Improved outcomes with early diagnosis
* Chorionicity is the strongest predictor
* Higher neonatal morbidity compared to singleton pregnancy
---
## **14. Key Clinical Pearls**
* Early determination of chorionicity is critical
* Monochorionic twins require closer surveillance
* Preterm birth is the most common complication
* Delivery planning should be individualized
---
If you want, I can next provide:
**25 hard case-based MCQs (HTML CSS JS single file)**, **FAQs for SEO**, or **exam-oriented short notes** for twin pregnancy.