Placenta Accreta Spectrum: Definition, Risk Factors, Diagnosis and Management
Below is a **fully SEO-optimized, image-free, exam-ready and clinically complete** article on **Placenta Accreta Spectrum**, structured exactly in the **H1 → H2 → H3** format that search engines and medical readers prefer.
---
## **SEO Title**
**Placenta Accreta Spectrum: Definition, Risk Factors, Diagnosis and Management**
---
## **SEO Meta Description**
Comprehensive clinical guide on Placenta Accreta Spectrum covering definition, types, pathophysiology, risk factors, diagnosis, imaging criteria, antenatal planning, surgical management, complications, and maternal outcomes.
---
## **SEO Keywords**
placenta accreta spectrum, placenta accreta, placenta increta, placenta percreta, morbidly adherent placenta, placenta accreta diagnosis, placenta accreta ultrasound signs, placenta accreta MRI, placenta accreta management, cesarean hysterectomy accreta, postpartum hemorrhage accreta
---
# **Placenta Accreta Spectrum**
## **1. Definition**
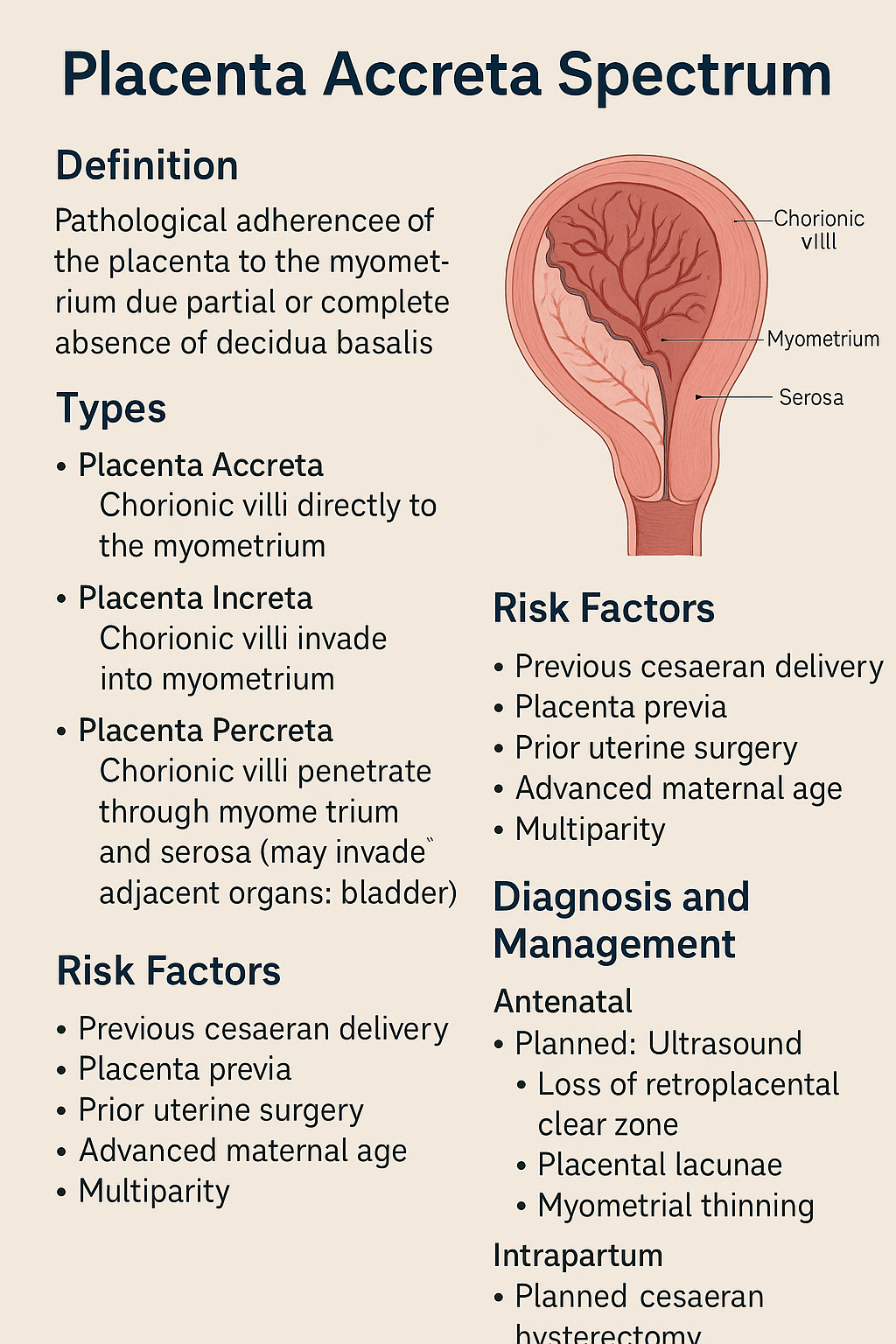
Placenta Accreta Spectrum (PAS) refers to a group of abnormal placental attachment disorders characterized by **pathological adherence of the placenta to the myometrium due to partial or complete absence of decidua basalis**, resulting in failure of normal placental separation after delivery.
---
## **2. Classification of Placenta Accreta Spectrum**
### **2.1 Placenta Accreta**
* Chorionic villi attach **directly to the myometrium**
* Most common and least severe form
### **2.2 Placenta Increta**
* Chorionic villi **invade into the myometrium**
### **2.3 Placenta Percreta**
* Chorionic villi **penetrate through the myometrium and serosa**
* May invade adjacent organs (bladder most commonly)
---
## **3. Epidemiology**
* Incidence: ~1 in 300–500 pregnancies
* Rapidly increasing due to rising cesarean section rates
* Major cause of **severe obstetric hemorrhage and maternal morbidity**
---
## **4. Etiopathogenesis and Pathophysiology**
### **4.1 Underlying Mechanism**
* Defective or absent decidua basalis
* Inadequate Nitabuch’s layer
* Direct trophoblastic invasion into myometrium
### **4.2 Contributing Factors**
* Prior uterine surgery leads to **endometrial scarring**
* Implantation over scar tissue promotes abnormal placental adherence
---
## **5. Risk Factors**
### **5.1 Major Risk Factors**
* Previous cesarean delivery (risk increases with number)
* Placenta previa with prior cesarean section
### **5.2 Additional Risk Factors**
* Previous myomectomy
* Dilatation and curettage
* Asherman syndrome
* Advanced maternal age
* Multiparity
* Assisted reproductive techniques
---
## **6. Clinical Features**
### **6.1 Antenatal Period**
* Often asymptomatic
* Frequently associated with placenta previa
* May present with painless antepartum bleeding
### **6.2 Intrapartum and Postpartum**
* Failure of placental separation
* Massive postpartum hemorrhage
* Hypovolemic shock
* Disseminated intravascular coagulation
---
## **7. Diagnosis**
### **7.1 Antenatal Diagnosis**
Early diagnosis is critical for reducing morbidity.
#### **Ultrasound (First Line)**
Key grayscale and Doppler findings:
* Loss of retroplacental clear zone
* Thinning of myometrium (<1 mm)
* Placental lacunae (“Swiss cheese” appearance)
* Turbulent lacunar blood flow
* Bridging vessels to bladder
#### **MRI (Adjunct Tool)**
Indications:
* Posterior placenta
* Suspected placenta percreta
* Inconclusive ultrasound
MRI Findings:
* Dark intraplacental bands on T2
* Myometrial thinning
* Uterine bulging
* Direct invasion of adjacent organs
---
## **8. Differential Diagnosis**
* Retained placenta
* Uterine atony
* Placenta previa without invasion
* Uterine inversion
---
## **9. Antenatal Management and Planning**
### **9.1 Multidisciplinary Approach**
* Obstetrician
* Anesthesiologist
* Interventional radiologist
* Urologist
* Blood bank support
### **9.2 Timing of Delivery**
* Planned delivery at **34–36 weeks**
* After corticosteroids for fetal lung maturity
### **9.3 Place of Delivery**
* Tertiary care center with massive transfusion capability
---
## **10. Intrapartum Management**
### **10.1 Preferred Surgical Approach**
* **Planned cesarean hysterectomy without attempting placental removal**
* Placenta left in situ to prevent catastrophic hemorrhage
### **10.2 Surgical Principles**
* Vertical uterine incision away from placenta
* Avoid placental manipulation
* Early hysterectomy following fetal delivery
---
## **11. Conservative Management Options**
Reserved for highly selected cases desiring fertility.
### **11.1 Methods**
* Placenta left in situ
* Uterine artery embolization
* Methotrexate use (controversial)
### **11.2 Risks**
* Severe infection
* Delayed hemorrhage
* Secondary hysterectomy
---
## **12. Complications**
### **12.1 Maternal Complications**
* Massive hemorrhage
* Blood transfusion reactions
* Bladder or ureteric injury
* Sepsis
* Thromboembolism
* Maternal mortality
### **12.2 Fetal Complications**
* Prematurity
* Low birth weight
* NICU admission
---
## **13. Prognosis**
* Prognosis improves significantly with **antenatal diagnosis**
* Planned surgery reduces maternal mortality
* Future fertility usually lost with definitive surgery
---
## **14. Prevention**
* Rational use of cesarean sections
* Avoid unnecessary uterine curettage
* Early risk stratification in placenta previa cases
---
## **15. Key Exam and Clinical Pearls**
* Placenta previa with previous cesarean = **PAS until proven otherwise**
* Never attempt manual placental removal if accreta suspected
* Cesarean hysterectomy is the gold standard management
* MRI complements ultrasound, not a replacement
---
If you want, I can next provide:
* **Case-based MCQs (HTML CSS JS single file)**
* **PAS vs Placenta Previa comparison table**
* **FAQ section for SEO**
* **Schema-ready JSON-LD medical article**
Just tell me 👍