Induction of Labor Indications Methods Contraindications Complications
Below is a **concise yet complete, SEO-friendly, exam-ready reference** on **Induction of Labor**, structured with clear headings (H1–H3 style) and high-yield clinical content.
---
# **Induction of Labor**
## **Definition**
**Induction of labor (IOL)** is the **artificial initiation of uterine contractions** before the spontaneous onset of labor, with the aim of achieving **vaginal delivery**, when continuation of pregnancy poses **greater maternal or fetal risk** than delivery.
---
## **Indications for Induction of Labor**
### **Maternal Indications**
* Post-term pregnancy (≥41 weeks)
* Pre-eclampsia and eclampsia
* Gestational hypertension
* Diabetes mellitus (gestational or pre-existing)
* Premature rupture of membranes (PROM) at term
* Chorioamnionitis
* Rh isoimmunization
* Maternal medical disorders (renal, cardiac disease)
* Intrauterine fetal demise (IUFD)
### **Fetal Indications**
* Intrauterine growth restriction (IUGR)
* Oligohydramnios
* Non-reassuring fetal status (controlled setting)
* Fetal anomalies requiring early delivery
### **Elective Induction**
* At ≥39 weeks with confirmed gestational age and favorable cervix
---
## **Contraindications to Induction of Labor**
### **Absolute Contraindications**
* Placenta previa
* Vasa previa
* Transverse lie
* Cord prolapse
* Previous classical cesarean section
* Previous uterine rupture
* Invasive cervical cancer
* Cephalopelvic disproportion (CPD)
### **Relative Contraindications**
* Multiple previous cesarean sections
* Grand multiparity
* Unstable lie
* Active genital herpes
---
## **Pre-Induction Assessment**
Show readiness of cervix and maternal-fetal safety.
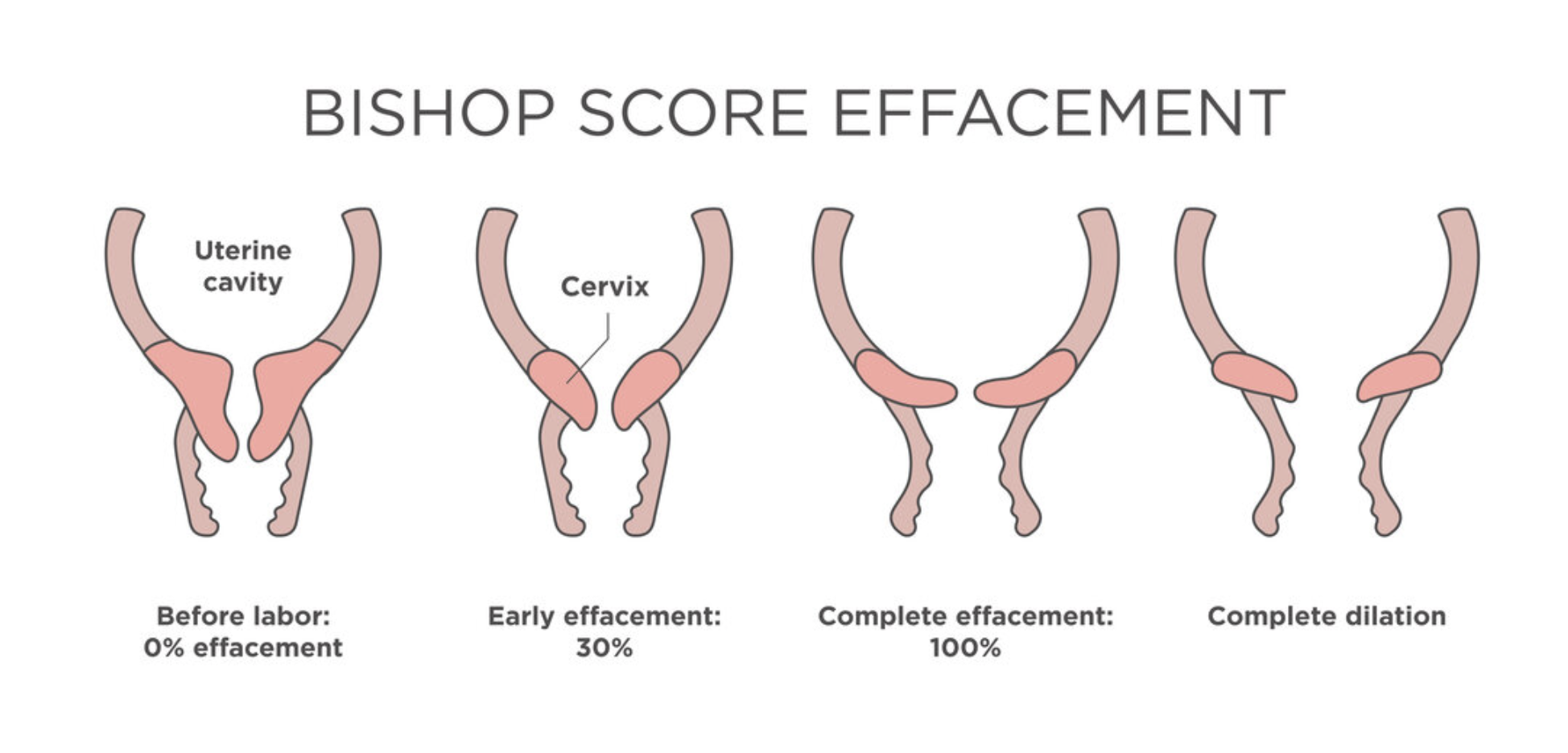
### **Bishop Score**
Assesses **cervical favorability** using:
* Cervical dilatation
* Effacement
* Consistency
* Position
* Fetal station
**Score interpretation:**
* **≥6–8** → Favorable cervix (high success)
* **<6** → Unfavorable cervix (requires cervical ripening)
---
## **Methods of Induction of Labor**
### **1. Mechanical Methods**
* **Membrane sweeping**
* **Foley catheter (balloon catheter)**
* Double balloon catheter
**Advantages:** Low cost, minimal uterine hyperstimulation
**Disadvantages:** Discomfort, infection risk
---
### **2. Pharmacological Methods**
#### **Prostaglandins**
* **Dinoprostone (PGE₂)** – Gel, tablet, vaginal insert
* **Misoprostol (PGE₁)** – Oral or vaginal
**Actions:**
* Cervical ripening
* Uterine contractions
**Contraindications:**
* Previous uterine scar (relative for misoprostol)
* Fetal distress
* Hypersensitivity
---
#### **Oxytocin**
* Used after cervical ripening
* IV infusion with titration
**Mechanism:** Stimulates uterine smooth muscle contraction
**Monitoring:** Continuous CTG required
---
### **3. Surgical Methods**
* **Amniotomy (Artificial rupture of membranes)**
**Prerequisites:**
* Engaged head
* Favorable cervix
* No placenta previa
---
## **Monitoring During Induction**
* Continuous fetal heart rate monitoring
* Maternal vitals
* Uterine contraction pattern
* Progress of labor (partograph)
---
## **Complications of Induction of Labor**
### **Maternal Complications**
* Uterine hyperstimulation
* Uterine rupture
* Postpartum hemorrhage
* Infection
* Failed induction leading to cesarean section
### **Fetal Complications**
* Fetal distress
* Meconium aspiration
* Birth asphyxia
* Cord prolapse (after amniotomy)
---
## **Failed Induction**
**Definition:** Failure to establish active labor after adequate attempts with appropriate methods.
**Management:**
* Re-assess indication
* Repeat cervical ripening
* Cesarean delivery if indicated
---
## **Key Clinical Pearls**
* Always confirm **gestational age** before induction
* Bishop score guides method selection
* Avoid prostaglandins in scarred uterus (especially misoprostol)
* Continuous monitoring is mandatory
* Individualize induction based on maternal and fetal condition
---
## **Conclusion**
Induction of labor is a **critical obstetric intervention** that improves maternal and fetal outcomes when appropriately indicated. Proper **case selection, cervical assessment, method choice, and vigilant monitoring** are essential to maximize success and minimize complications.
---
If you want, I can next provide:
* **SEO title, meta description, and keywords**
* **Exam-oriented tables**
* **Case-based MCQs (HTML + CSS + JS, single file, modern UI)**
* **Flowcharts for induction decision-making**