Ectopic Pregnancy: Causes, Symptoms, Diagnosis, Treatment Options Management Guidelines (2025 Complete Guide)
Below is a **single-place, exam-ready + clinical-practice detailed reference** on **Ectopic Pregnancy**, written in the **structured pattern you prefer** and suitable for your medical hub.
✔️ **No images included**
✔️ **Includes authoritative external links**
---
# **Ectopic Pregnancy – Complete Clinical & Management Guide (2025)**
---
## **1. Definition**
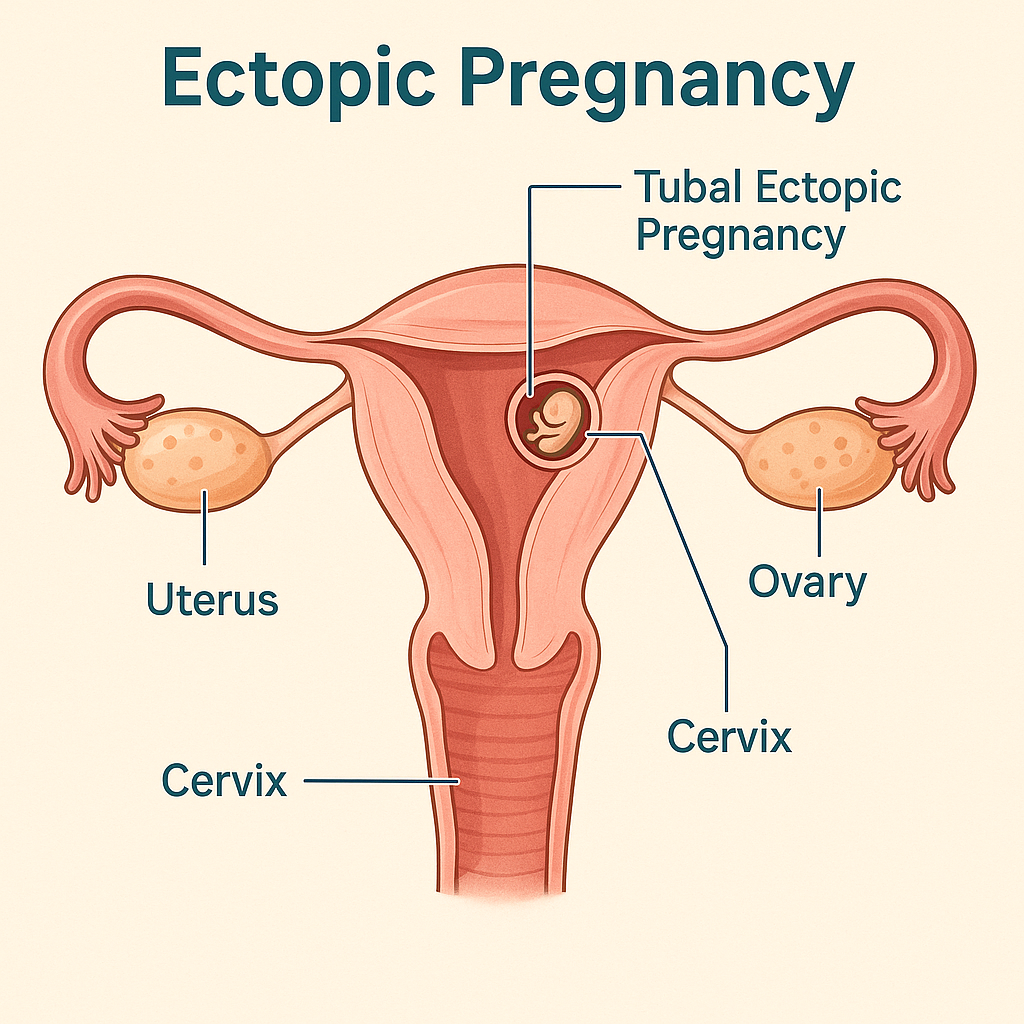
**Ectopic pregnancy** is implantation of a fertilized ovum **outside the endometrial cavity**.
> > 95% occur in the **fallopian tube**.
It is a **life-threatening obstetric emergency** if ruptured.
---
## **2. Epidemiology**
* Incidence: **1–2% of all pregnancies**
* Leading cause of **maternal mortality in first trimester**
* Rising incidence due to:
* Assisted reproductive techniques (ART)
* Pelvic inflammatory disease (PID)
---
## **3. Common Sites of Ectopic Pregnancy**
| Site | Approx. % |
| ---------------------- | ---------- |
| Ampullary tube | 70% |
| Isthmic tube | 12% |
| Fimbrial | 11% |
| Interstitial (cornual) | 2–4% |
| Ovarian | <1% |
| Cervical | <1% |
| Caesarean scar | Increasing |
---
## **4. Pathophysiology**
Normal embryo transport is impaired due to:
* **Tubal damage**
* **Altered tubal motility**
* **Delayed ovum transport**
→ Implantation occurs before reaching uterus
→ Trophoblastic invasion erodes vessels
→ **Tubal rupture → hemorrhage**
---
## **5. Risk Factors**
### High-risk
* Previous ectopic pregnancy
* Tubal surgery / sterilization
* PID (especially *Chlamydia*)
* Assisted reproduction (IVF)
### Moderate risk
* IUCD in situ
* Smoking
* Endometriosis
### No identifiable risk factor in ~50%
---
## **6. Clinical Features**
### Classical Triad (only ~50%)
1. **Amenorrhea**
2. **Lower abdominal pain**
3. **Vaginal bleeding**
### Other symptoms
* Shoulder tip pain (diaphragmatic irritation)
* Syncope
* Dizziness
### Signs of Rupture
* Hypotension
* Tachycardia
* Pallor
* Abdominal guarding
* Cervical motion tenderness
* Full, tender pouch of Douglas
---
## **7. Investigations / Diagnosis**
### 1. Urine Pregnancy Test
* Positive
### 2. Serum β-hCG (Quantitative)
* **Discriminatory zone**: ~1500–2000 IU/L
* If no intrauterine gestational sac → suspect ectopic
* Plateauing or suboptimal rise (<66% in 48 hrs)
### 3. Transvaginal Ultrasound (TVS)
**Suggestive findings**
* Empty uterus
* Adnexal mass
* Tubal ring sign
* Free fluid in pelvis
### 4. Culdocentesis (obsolete)
### 5. Diagnostic Laparoscopy (gold standard if uncertain)
---
## **8. Differential Diagnosis**
* Threatened / incomplete abortion
* Corpus luteum cyst
* Acute PID
* Ovarian torsion
* Appendicitis
* Renal colic
---
## **9. Management (Stepwise)**
### A. Expectant Management
**Criteria**
* Asymptomatic
* β-hCG <200 IU/L and declining
* No adnexal mass
* Reliable follow-up
---
### B. Medical Management – **Methotrexate**
#### Indications
* Hemodynamically stable
* Unruptured ectopic
* β-hCG ≤5000 IU/L
* No fetal cardiac activity
#### Contraindications
* Hemodynamic instability
* Liver, renal disease
* Breastfeeding
* Blood dyscrasias
#### Regimens
**Single-dose**
* Methotrexate **50 mg/m² IM**
* Check β-hCG on day 4 & 7
**Multi-dose**
* MTX 1 mg/kg on days 1,3,5,7
* Leucovorin rescue
---
### C. Surgical Management
#### Indications
* Ruptured ectopic
* Hemodynamic instability
* Failed medical treatment
* Contraindications to methotrexate
#### Procedures
* **Salpingectomy** (preferred if tube severely damaged)
* **Salpingostomy** (fertility preservation)
* Laparoscopy preferred over laparotomy (if stable)
---
## **10. Special Types**
### Interstitial (Cornual)
* Late rupture
* Massive hemorrhage
* Managed surgically ± MTX
### Cervical Ectopic
* Painless bleeding
* Managed with MTX, uterine artery embolization
### Caesarean Scar Pregnancy
* Increasing incidence
* High risk of placenta accreta
* Early MTX or surgical excision
---
## **11. Complications**
* Hemorrhagic shock
* Infertility
* Recurrent ectopic pregnancy
* Maternal death (if delayed)
---
## **12. Prognosis**
* Future fertility preserved in many
* Recurrence risk: **10–25%**
* Early diagnosis improves outcomes
---
## **13. Counselling & Follow-Up**
* Avoid pregnancy for **3 months after MTX**
* Early ultrasound in next pregnancy
* Discuss recurrence risk
* Rh-negative women → **Anti-D immunoglobulin**
---
## **14. Prevention**
* Prompt treatment of PID
* Smoking cessation
* Safe reproductive practices
* Early antenatal booking
---
## **15. Authoritative External Links**
* **WHO – Ectopic Pregnancy Overview**
[https://www.who.int](https://www.who.int)
* **ACOG Practice Bulletin: Tubal Ectopic Pregnancy**
[https://www.acog.org](https://www.acog.org)
* **RCOG Green-top Guideline No. 21**
[https://www.rcog.org.uk](https://www.rcog.org.uk)
* **UpToDate – Ectopic Pregnancy (Clinician Reference)**
[https://www.uptodate.com](https://www.uptodate.com)
* **NICE Guideline: Ectopic pregnancy and miscarriage**
[https://www.nice.org.uk](https://www.nice.org.uk)
---
If you want, I can next:
* Create **SEO title, meta description & keywords**
* Convert this into **HTML (single-file)** for your site
* Generate **case-based MCQs**
* Add **internal links** to abortion, PID, β-hCG interpretation, or early pregnancy bleeding
Just tell me 👍