covid 19
---
# **1. Definition**
COVID-19 is an acute viral disease caused by **SARS-CoV-2**, an enveloped, positive-sense **RNA coronavirus**. It ranges from asymptomatic infection to severe viral pneumonia, ARDS, sepsis, and multi-organ dysfunction.
---
# **2. Virology & Pathophysiology**
### **Virus**
* Betacoronavirus, 29–30 kb RNA genome.
* Structural proteins: **S (spike), E, M, N**.
* S-protein binds **ACE2** receptors + TMPRSS2 facilitates entry.
### **Host entry & organ tropism**
ACE2 found in:
* Type II alveolar cells
* Myocardium
* Endothelium
* GI mucosa
* Kidney proximal tubules
* CNS
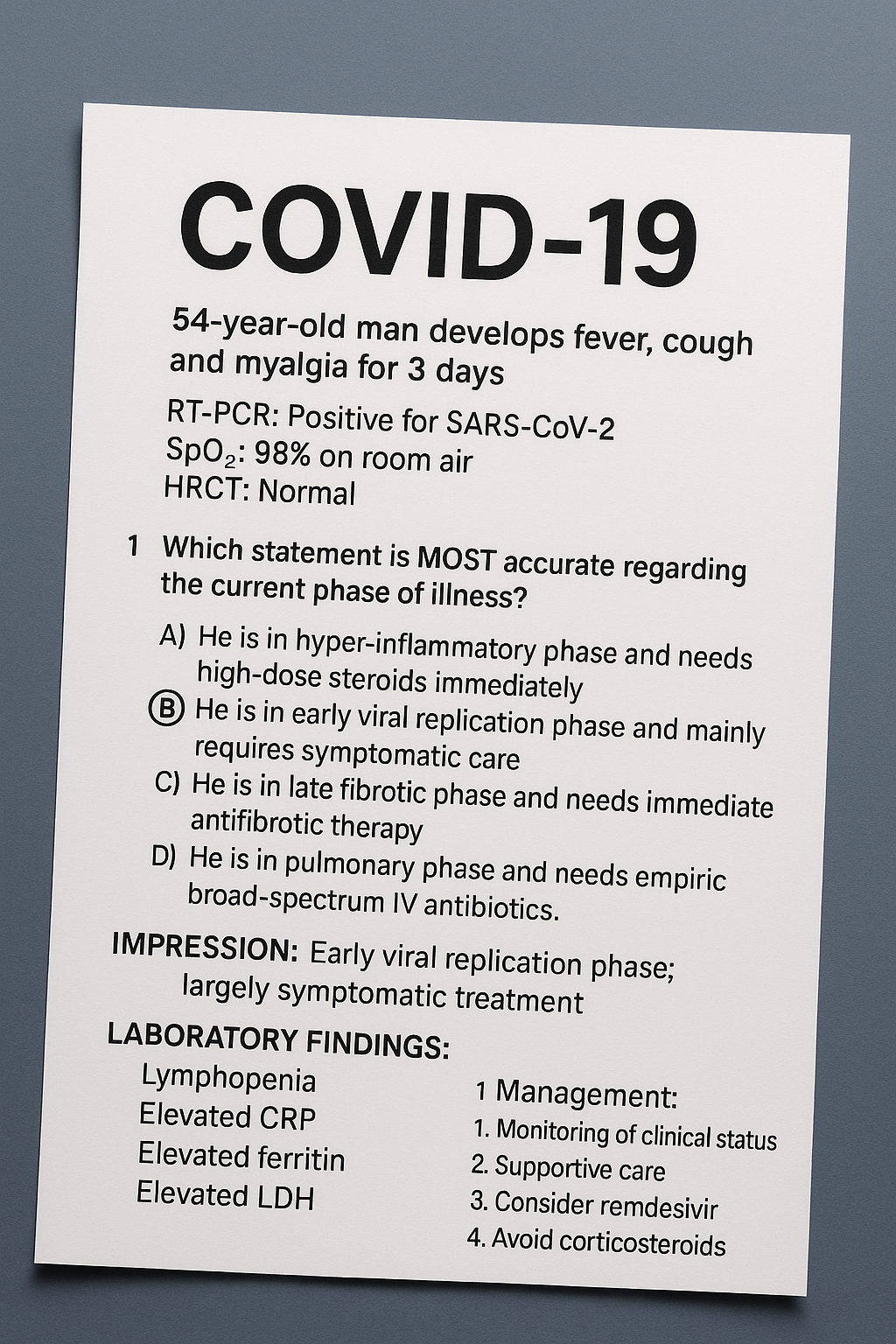
### **Phases of disease**
1. **Early Viral Replication Phase** (Days 1–5)
→ Viral replication high; symptoms mild; antivirals useful.
2. **Pulmonary Phase** (Days 5–10)
→ Viral + immune injury → pneumonia → hypoxia.
3. **Hyper-inflammatory Phase / Cytokine storm** (Days 10–14)
→ IL-6, IL-1β, TNF-α surge → ARDS, shock, thrombosis.
### **Immune Pathogenesis**
* Dysregulated innate immunity
* Delayed interferon response
* Hyper-inflammation
* **Endothelialitis + microvascular thrombosis** (↑ D-dimer)
* **Hypercoagulable state**
---
# **3. Modes of Transmission**
* Respiratory droplets, aerosols
* Fomites (less common)
* Close contact
* Vertical transmission rare
* Highest contagious period: **2 days before and 3 days after symptom onset**.
---
# **4. Variants (Updated Classification)**
* **Alpha, Beta, Gamma** — earlier waves
* **Delta** — more severe, high hospitalization
* **Omicron (BA.1 → BA.5, XBB, BQ, JN.1)** — highly transmissible, less severe, immune evasion
* **Current dominant lineages (global): Omicron sublineages** with high reinfection capability.
---
# **5. Clinical Features**
### **Asymptomatic:** ~30–40%
### **Mild (Upper respiratory)**
* Fever, dry cough
* Sore throat
* Anosmia/ageusia
* Rhinorrhea
* Myalgia, fatigue
### **Moderate**
* Pneumonia with **SpO₂ ≥ 94%**
* Dyspnea
* Persistent fever
### **Severe**
* **SpO₂ < 94%**
* RR ≥ 30/min
* Lung infiltrates > 50%
* Respiratory distress
### **Critical**
* ARDS
* Septic shock
* Multi-organ dysfunction
* Acute cardiac injury
* Acute kidney injury
### **Complications**
* ARDS
* Cytokine storm
* Microthrombosis, DVT, PE
* MIS-C (children)
* Myocarditis
* Acute liver injury
* Long COVID (fatigue, dyspnea, cognitive dysfunction)
---
# **6. Investigations**
### **Baseline**
* CBC: lymphopenia
* CRP: ↑
* D-dimer: ↑
* Ferritin: ↑
* LDH: ↑
* LFT, RFT
* ABG (if hypoxic)
### **Radiology**
**HRCT chest findings**:
* Bilateral peripheral **ground-glass opacities**
* Crazy-paving pattern
* Patchy consolidation
* CT Severity Score (CSS) used for monitoring
### **Diagnostic Tests**
* **RT-PCR (gold standard)**
* Genes: RdRp, N, E
* Ct < 25 → high viral load
* **Rapid Antigen Test** (moderate sensitivity)
* **Serology IgM/IgG** (past infection)
---
# **7. Differential Diagnosis**
* Influenza
* RSV
* Adenovirus pneumonia
* Bacterial pneumonia
* Pulmonary embolism
* Heart failure
* Other viral pneumonias (CMV, H1N1)
---
# **8. Management (Stepwise)**
---
# 🟢 **A. Mild COVID-19 (Home Care)**
* Paracetamol
* Hydration
* Pulse oximeter monitoring
* Zinc (optional)
* Avoid steroids
* **Antivirals only for high-risk** (elderly, comorbid, immunosuppressed):
* **Nirmatrelvir + Ritonavir (Paxlovid)**
* **Remdesivir (early 3-day outpatient regimen)**
---
# 🟡 **B. Moderate (SpO₂ ≥ 94% but pneumonia present)**
* **Oxygen if required** (target 92–96%)
* **Steroids: Dexamethasone 6 mg/day**
* **Remdesivir**
* **Anticoagulation: Enoxaparin prophylactic dose**
* Monitor:
* CRP, D-dimer
* RR, SpO₂ trends
* Chest imaging if worsening
---
# 🔴 **C. Severe / Critical COVID-19**
### **1. Respiratory**
* Oxygen: NRBM → HFNC → NIV
* Intubation for refractory hypoxia
* Proning (awake & ventilated)
### **2. Anti-inflammatory**
* Dexamethasone 6 mg IV/PO x 10 days
* **Tocilizumab** (IL-6 inhibitor) for cytokine storm
* Baricitinib (JAK inhibitor) when Tocilizumab unavailable
### **3. Anticoagulation**
* **Therapeutic enoxaparin** in high D-dimer or suspected thrombosis
* Avoid if bleeding risk
### **4. Antivirals**
* Remdesivir (if < 10 days from symptom onset)
* Paxlovid (early disease only)
### **5. Organ Support**
* Vasopressors
* Renal replacement therapy
* ECMO in selected cases
---
# **9. Pharmacology of Key Drugs**
*(Indication, MOA, Dosage, PK, ADRs, Contra, Monitoring, Counselling)*
---
## **A. Remdesivir**
**Indication:** Moderate–severe COVID (within 10 days of symptoms)
**MOA:** RNA-dependent RNA polymerase inhibitor
**Dose:**
* 200 mg IV day 1 → 100 mg IV daily × 5 days
**PK:** Hepatic metabolism; renal elimination
**ADRs:** LFT elevation, bradycardia
**Contra:** GFR < 30 ml/min
**Monitoring:** LFT, renal function
**Counselling:** Report palpitations, yellowing of eyes.
---
## **B. Dexamethasone**
**Indication:** Hypoxic COVID
**MOA:** Corticosteroid → suppresses cytokine storm
**Dose:** 6 mg/day PO/IV (max 10 days)
**ADRs:** Hyperglycemia, secondary infection, GI bleed
**Contra:** Uncontrolled diabetes, active fungal infection
**Monitoring:** RBS, BP, sepsis signs
**Counselling:** Take with food, watch for fever/worsening cough.
---
## **C. Tocilizumab**
**Indication:** Severe COVID with high IL-6/CRP
**MOA:** IL-6 receptor blocker
**Dose:** 8 mg/kg IV single dose (max 800 mg)
**ADRs:** Hepatitis, neutropenia, bowel perforation
**Contra:** Sepsis, TB
**Monitoring:** LFT, CBC, CRP
**Counselling:** Report abdominal pain, jaundice.
---
## **D. Nirmatrelvir + Ritonavir (Paxlovid)**
**Indication:** High-risk mild/moderate COVID **within 5 days**
**MOA:** 3CL protease inhibition + ritonavir boosting
**Dose:** 300 mg/100 mg BID × 5 days
**PK:** CYP3A4 inhibition (many interactions!)
**ADRs:** Dysgeusia, diarrhea
**Contra:** Statins, antiarrhythmics, immunosuppressants
**Monitoring:** Drug interactions, renal function
**Counselling:** Bitter taste normal; keep hydration.
---
## **E. Enoxaparin**
**Indication:** Hypercoagulability in COVID
**MOA:** Inhibits factor Xa
**Dose:**
* Prophylactic: 40 mg SC daily
* Therapeutic: 1 mg/kg SC BID
**ADRs:** Bleeding, HIT
**Contra:** Active bleeding
**Monitoring:** Platelets, PT/aPTT
**Counselling:** Look for bruising.
---
# **10. MIS-C (Children)**
* Persistent fever
* Multisystem inflammation
* Rash, shock, myocarditis
**Treatment:** IVIG + steroids + aspirin.
---
# **11. Long COVID**
Symptoms > 12 weeks:
* Fatigue
* Breathlessness
* Brain fog
* Autonomic dysfunction
* Depression/anxiety
**Management:**
Rehab, pulmonary exercises, sleep hygiene, CBT if needed.
---
# **12. Prevention**
### **General**
* Masks
* Ventilation
* Hand hygiene
* Avoid crowded indoor spaces
### **Vaccination**
Approved platforms:
* mRNA (Pfizer, Moderna)
* Viral vector (Covishield, AstraZeneca, J&J)
* Inactivated (Covaxin, Sinopharm)
* Protein subunit (Novavax)
**Booster indicated** for elderly, comorbid, immunocompromised.
---
# **13. Key Exam Pearls**
* **RT-PCR Ct value does NOT correlate with severity.**
* **Steroids only in hypoxia.**
* **Remdesivir not useful late (>10 days).**
* **Tocilizumab only with high inflammatory markers.**
* **High D-dimer is a poor prognostic marker.**
* **Omicron → less LRT disease but high reinfection rates.**
---