Antepartum Hemorrhage (APH): Causes, Symptoms, Diagnosis, Management and Complications
---
# **Antepartum Hemorrhage (APH): Causes, Symptoms, Diagnosis, Management and Complications**
---
## **What Is Antepartum Hemorrhage?**
### **Definition of Antepartum Hemorrhage**
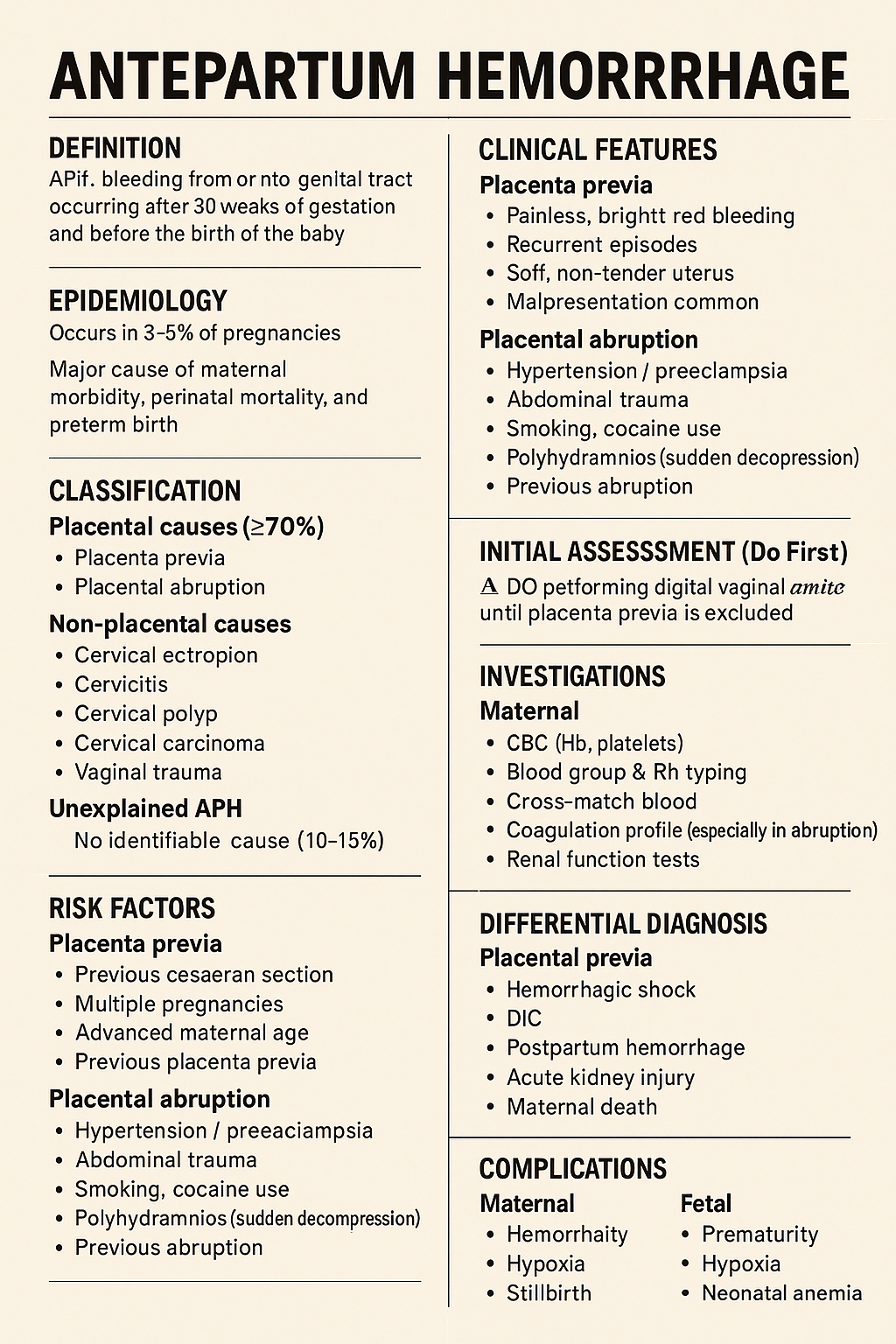
Antepartum hemorrhage (APH) is defined as **bleeding from or into the genital tract occurring after 20 weeks of gestation and before the delivery of the fetus**.
### **Meaning of APH in Pregnancy**
APH is a **major obstetric emergency** associated with significant **maternal morbidity, fetal hypoxia, preterm birth, and perinatal mortality**.
---
## **Epidemiology of Antepartum Hemorrhage**
### **Incidence of APH**
* Occurs in **3–5% of all pregnancies**
* Accounts for a large proportion of **emergency obstetric admissions**
### **Maternal and Perinatal Impact**
* Major cause of:
* Maternal anemia
* Hemorrhagic shock
* Stillbirth
* Neonatal intensive care admission
---
## **Classification of Antepartum Hemorrhage**
### **Placental Causes of Antepartum Hemorrhage**
Placental causes account for **approximately 70% of APH cases**.
#### **Placenta Previa**
Placenta implanted in the **lower uterine segment**, partially or completely covering the internal cervical os.
#### **Placental Abruption (Abruptio Placentae)**
Premature separation of a **normally situated placenta** after 20 weeks of gestation.
#### **Vasa Previa**
Fetal blood vessels traverse the membranes over the cervical os, unprotected by placenta or Wharton’s jelly.
---
### **Non-Placental Causes of Antepartum Hemorrhage**
#### **Cervical Causes**
* Cervical ectropion
* Cervicitis
* Cervical polyps
* Cervical carcinoma
#### **Vaginal Causes**
* Trauma
* Infection
* Varicosities
---
### **Unexplained Antepartum Hemorrhage**
* No identifiable cause
* Occurs in **10–15%** of cases
* Still associated with adverse fetal outcomes
---
## **Risk Factors for Antepartum Hemorrhage**
### **Risk Factors for Placenta Previa**
* Previous cesarean section
* Previous placenta previa
* Multiparity
* Advanced maternal age
* Smoking
### **Risk Factors for Placental Abruption**
* Hypertension and preeclampsia
* Abdominal trauma
* Smoking and cocaine use
* Polyhydramnios
* Sudden uterine decompression
---
## **Pathophysiology of Antepartum Hemorrhage**
### **Pathophysiology of Placenta Previa**
* Placenta in lower uterine segment
* Stretching and thinning cause **placental separation**
* Results in **painless bleeding**
### **Pathophysiology of Placental Abruption**
* Rupture of maternal vessels in decidua basalis
* Formation of retroplacental hematoma
* Leads to **uterine hypertonicity and fetal hypoxia**
### **Pathophysiology of Vasa Previa**
* Rupture of fetal vessels
* Rapid fetal blood loss
* Can cause **acute fetal demise**
---
## **Clinical Features of Antepartum Hemorrhage**
### **General Symptoms of APH**
* Vaginal bleeding
* Reduced fetal movements
* Abdominal pain (may or may not be present)
---
### **Clinical Features of Placenta Previa**
* **Painless**, bright red bleeding
* Recurrent episodes
* Soft, non-tender uterus
* Malpresentation common
* Fetal heart sounds usually normal
---
### **Clinical Features of Placental Abruption**
* **Painful bleeding**
* Dark blood
* Tense, tender uterus
* Maternal shock may be disproportionate
* Fetal distress or absent heart sounds
---
### **Clinical Features of Vasa Previa**
* Sudden bleeding after rupture of membranes
* Fetal bradycardia
* Maternal condition relatively stable
---
## **Initial Assessment of Antepartum Hemorrhage**
### **Primary Survey (ABC Approach)**
* Airway, Breathing, Circulation
* Oxygen supplementation
* Two large-bore IV cannulae
* Monitor vitals and urine output
### **Important Clinical Rule**
⚠️ **Digital vaginal examination is contraindicated until placenta previa is excluded**
---
## **Investigations in Antepartum Hemorrhage**
### **Laboratory Investigations**
* Complete blood count
* Blood group and Rh typing
* Cross-match blood
* Coagulation profile (especially in abruption)
* Renal function tests
---
### **Imaging in Antepartum Hemorrhage**
* **Ultrasound** for placental localization
* Doppler ultrasound for suspected vasa previa
* Continuous CTG for fetal monitoring
---
## **Differential Diagnosis of Antepartum Hemorrhage**
* Placenta previa
* Placental abruption
* Vasa previa
* Preterm labor with show
* Cervical malignancy
* Uterine rupture (rare)
---
## **Management of Antepartum Hemorrhage**
### **General Management Principles**
* Hospital admission
* Bed rest
* IV fluids
* Blood transfusion if required
* Anti-D immunoglobulin for Rh-negative mothers
* Corticosteroids if gestation <34 weeks
---
## **Management of Placenta Previa**
### **Expectant Management**
Indicated when:
* Bleeding is mild
* Gestation is preterm
* Mother and fetus stable
Includes:
* Close monitoring
* Avoid vaginal exams
* Steroids for fetal lung maturity
---
### **Definitive Management**
* **Cesarean section** is the mode of delivery for:
* Major placenta previa
* Heavy or recurrent bleeding
* Fetal distress
* Term pregnancy
---
## **Management of Placental Abruption**
### **Mild Abruption**
* Conservative management
* Close maternal and fetal monitoring
### **Severe Abruption**
* Immediate delivery
* Blood products
* Correction of coagulopathy
### **Mode of Delivery**
* Vaginal if fetus dead and labor progressing
* Cesarean if fetus alive with distress
---
## **Management of Vasa Previa**
* Emergency cesarean section
* Neonatal resuscitation readiness
* Planned elective cesarean if diagnosed antenatally
---
## **Complications of Antepartum Hemorrhage**
### **Maternal Complications**
* Hemorrhagic shock
* Disseminated intravascular coagulation (DIC)
* Postpartum hemorrhage
* Acute kidney injury
* Maternal death
---
### **Fetal Complications**
* Prematurity
* Intrauterine growth restriction
* Fetal hypoxia
* Stillbirth
* Neonatal anemia
---
## **Prevention of Antepartum Hemorrhage**
### **Preventive Strategies**
* Routine antenatal ultrasound
* Control of hypertension
* Avoid smoking and substance abuse
* Planned delivery in high-risk pregnancies
---
## **Prognosis of Antepartum Hemorrhage**
### **Maternal Prognosis**
* Good with early diagnosis and prompt management
### **Fetal Prognosis**
* Depends on:
* Cause of APH
* Gestational age
* Speed of intervention
---
## **Exam-Oriented Key Points**
* **Painless bleeding → Placenta previa**
* **Painful bleeding + tender uterus → Abruption**
* **Shock out of proportion → Concealed abruption**
* **Never perform PV exam before ruling out placenta previa**
---
## **Frequently Asked Questions (SEO Boost)**
### **Is antepartum hemorrhage dangerous?**
Yes. APH is a **medical emergency** that can threaten both maternal and fetal life.
### **What is the most common cause of APH?**
**Placenta previa** is the most common cause.
### **Can APH be prevented?**
Some causes can be reduced with proper antenatal care and risk factor control.
---